Have A Day Transfusion? Your Complete Guide To Same-Day Blood Transfusions
Have you or a loved one been told you need a day transfusion? The phrase can sound clinical and intimidating, sparking a flood of questions: What exactly does it involve? Is it safe to go home the same day? How do I prepare? You're not alone in wondering. Many patients facing the need for a blood transfusion are now offered a modern, efficient approach called a same-day transfusion or outpatient transfusion. This guide demystifies the entire process, from the initial doctor's recommendation to walking out the clinic door feeling better, all within a single day. We’ll explore the medical science, the practical logistics, the benefits, and address every common concern you might have about this increasingly common medical procedure.
Understanding the Modern "Day Transfusion" Concept
What Exactly Is a Same-Day or Outpatient Transfusion?
A day transfusion, formally known as a same-day outpatient blood transfusion, is a precisely coordinated medical procedure where a patient receives donated blood or blood components in a hospital outpatient department, infusion center, or specialized clinic and is discharged to go home on the very same day. It stands in contrast to the traditional model of inpatient transfusion, which requires a hospital admission, often for one or more nights. This model is built on a foundation of stringent safety protocols, advanced monitoring technology, and a deep understanding of which patients are suitable candidates. The entire journey—from check-in through the transfusion itself and a final observation period—typically spans 4 to 8 hours. This approach has revolutionized care for patients with chronic conditions like myelodysplastic syndromes (MDS), aplastic anemia, thalassemia, or those experiencing chemotherapy-induced anemia, allowing them to avoid the disruption and cost of a hospital stay.
The Critical Role of Patient Selection and Safety
Not every patient is an automatic candidate for a day transfusion. Medical teams conduct a thorough evaluation to ensure safety. Key criteria often include:
- The Helmut Huber Scandal Leaked Videos Reveal His Hidden Porn Past
- Stuart Mad Tv Leak Secret Video Reveals His Darkest Secret
- Ratatata74
- Stable Vital Signs: The patient must have normal or well-controlled blood pressure, heart rate, and temperature.
- No Active Infection: Transfusions are postponed if the patient has a fever or signs of systemic infection.
- Adequate Vascular Access: Access is typically via a peripheral IV in the arm. Patients with difficult venous access may require a more complex assessment.
- No History of Severe Transfusion Reactions: A history of severe allergic, hemolytic, or transfusion-related acute lung injury (TRALI) reactions usually precludes outpatient settings.
- Reliable Transportation and Support: The patient must have a dedicated adult driver and cannot drive themselves. They must also have a responsible adult companion at home for the first 24 hours.
- Proximity to Care: Living within a reasonable distance (often 30-60 minutes) from the transfusion center is mandatory in case of a delayed reaction.
This meticulous screening is the cornerstone of making same-day transfusion a safe and viable option for thousands of patients annually.
The Medical Conditions That Often Lead to a Day Transfusion
Chronic Anemia and Bone Marrow Disorders
For patients with chronic anemias—such as those caused by kidney disease, inflammatory bowel disease (IBD), or bone marrow failure syndromes like MDS—regular red blood cell transfusions are a lifeline to combat fatigue, shortness of breath, and weakness. The predictability of their condition and the typically slow, steady nature of their anemia make them ideal candidates for the outpatient transfusion model. Instead of spending days in a hospital bed, they can schedule their "transfusion appointment" like any other medical visit, receive their units of packed red blood cells, and return home to rest in their own bed, resuming light activities the next day. This model dramatically improves quality of life and reduces the psychological burden of being a "hospital patient."
Oncology and Chemotherapy Support
Cancer treatments, particularly certain chemotherapy regimens and radiation therapy, can severely suppress bone marrow function, leading to dangerous drops in red blood cells (anemia) and platelets (thrombocytopenia). While platelet transfusions are often given in hospitals due to a slightly higher risk of reaction, red blood cell transfusions for cancer-related anemia are very commonly performed as day transfusions. This allows patients to avoid long hospital stays between treatment cycles, minimizing disruption to their personal lives, work, and family responsibilities. It represents a shift toward patient-centered cancer care, treating the whole person, not just the disease.
Pre-Operative Optimization and Acute Blood Loss
Sometimes, a day transfusion is used strategically before a planned surgery to correct pre-existing anemia, improving surgical outcomes and reducing the need for transfusions during the operation itself. Additionally, for patients who have experienced a moderate but stabilized acute blood loss (e.g., from a gastrointestinal ulcer that has been endoscopically treated), a same-day transfusion can restore blood volume and oxygen-carrying capacity without necessitating a full admission. The decision hinges on the patient's stability and the expected trajectory of their recovery.
- Cookie The Monsters Secret Leak Nude Photos That Broke The Internet
- Gary Lockwoods Sex Scandal Leak How It Destroyed His Life
- The Viral Scandal Kalibabbyys Leaked Nude Photos That Broke The Internet
Preparing for Your Day Transfusion: A Step-by-Step Checklist
The Pre-Transfusion Workup (Days/Weeks Before)
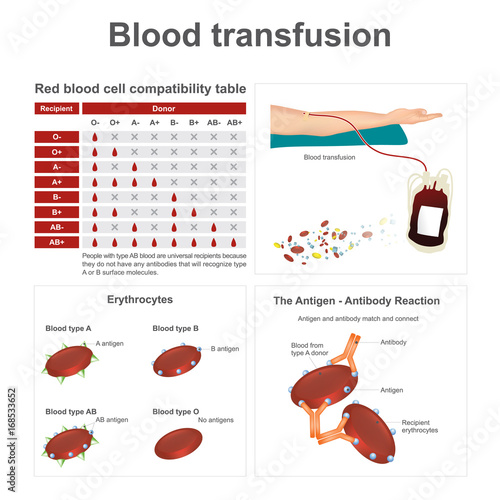
Preparation begins long before you arrive at the infusion center. Your hematologist or ordering physician will order a type and crossmatch test. This is a critical lab work that determines your ABO blood group and Rh factor, and then identifies specific donor blood units that are compatible with your unique blood profile. This process can take 1-3 days. You will also need a recent complete blood count (CBC) to confirm the need for transfusion (e.g., hemoglobin level below a certain threshold, often <7-8 g/dL for stable outpatients). It's crucial to inform your care team of all medications, especially anticoagulants (like warfarin, DOACs) or antiplatelet drugs (like aspirin, clopidogrel), as some may need to be held. Discuss any history of transfusion reactions, allergies, or heart failure, as these impact fluid management during the transfusion.
The Day Of: What to Bring and How to Behave
On the day of your day transfusion, your goal is to be comfortable and compliant.
- What to Bring: A valid photo ID, your insurance card, a list of current medications, any required co-pays, and entertainment (tablet, book, headphones). Wear comfortable, loose-fitting clothing with sleeves that can easily roll up above the elbow.
- Hydration is Key: Drink plenty of clear fluids (water, clear juice) before arriving. Good hydration makes IV insertion easier and helps your body process the additional fluid volume from the blood product.
- Nutrition: Eat a light, healthy meal or snack beforehand. Do not arrive fasting unless specifically instructed.
- Medications: Take your regular daily medications as prescribed, unless your doctor said otherwise. Do not take any new over-the-counter medications or supplements without checking.
- Companion: Your driver/companion must accompany you to check-in and will be asked to provide contact information. They will stay with you or be on-call nearby.
Inside the Infusion Center: The Transfusion Experience
Check-In, Vital Signs, and IV Placement
Upon arrival, you'll complete check-in paperwork. A nurse will then escort you to a comfortable recliner or bed in the infusion suite. The first step is taking your vital signs (temperature, blood pressure, pulse, respiratory rate) to establish a baseline. The nurse will then attempt to place a peripheral intravenous (IV) catheter, usually in your arm or hand. This is the most variable part of the experience; for some, it's quick and easy, for others with "hard-to-find veins," it may take a few tries. Applying a warm compress to the intended site before arrival can help dilate veins. Once the IV is secure and flushed with saline, the blood unit—which has been meticulously checked against your identity and medical record by two separate clinicians—is connected via a special blood administration set with a filter.
The Transfusion Itself: Monitoring and Milestones
The transfusion begins slowly. For the first 15 minutes, the rate is kept very low (often 2 mL/minute). This is the critical period for detecting acute reactions. The nurse will remain with you, frequently checking your vital signs and asking how you feel. If all is well after this initial period, the rate is increased to a standard flow (typically completing one unit in 2-4 hours). You will receive pre-medications (like acetaminophen or an antihistamine) only if you have a history of minor reactions or if your doctor anticipates one; routine pre-medication for all patients is not recommended by guidelines as it can mask early signs of a reaction. During the transfusion, you can read, watch TV, use your phone, or sleep. The nurse will perform vital sign checks at regular intervals (e.g., every 30-60 minutes). You must immediately alert the nurse if you feel any new symptoms: fever, chills, itching, hives, back pain, shortness of breath, chest pain, or a sense of impending doom.
The Final Observation Period and Discharge
Once the last drop of blood has been administered, the IV is flushed with saline and removed. You are not discharged immediately. A minimum 30-60 minute observation period is required after the transfusion ends to monitor for delayed hemolytic or allergic reactions, which can occur even after the blood is finished. During this time, your final set of vital signs is taken. If everything is stable, the nurse will provide you with written discharge instructions. These are crucial and typically include:
- Symptoms to watch for at home (fever >100.4°F, chills, dark urine, jaundice, difficulty breathing, rash).
- Activity recommendations (avoid heavy lifting or strenuous exercise for 24 hours).
- Hydration advice (continue drinking fluids).
- When to resume normal medications.
- A 24-hour emergency contact number for the transfusion center or hospital.
You must be discharged with your companion; you will not be allowed to leave alone or drive.
The Tangible Benefits of Choosing a Day Transfusion
For Patients: Convenience, Comfort, and Autonomy
The advantages for patients are profound. The most obvious is convenience. A procedure that once required a 2-3 day hospital stay is now a single-day outpatient appointment. This translates to less time away from work, family, and daily routines. Comfort is another major factor. Recovering in a quiet home environment, in your own bed, with familiar foods and routines, is vastly preferable to a noisy hospital room with frequent interruptions. Psychologically, it helps maintain a sense of normalcy and autonomy, reducing the "sick role" identity that can accompany prolonged hospitalizations. For patients with chronic conditions requiring regular transfusions (e.g., every 3-4 weeks), this model can mean dozens of extra days of "normal life" each year.
For the Healthcare System: Efficiency and Resource Stewardship
From a systemic perspective, day transfusions are a cornerstone of value-based care. They significantly reduce healthcare costs by freeing up expensive inpatient beds for those who truly need them. It optimizes the use of clinical staff, infusion chairs, and blood bank resources. Studies have shown that carefully selected outpatient transfusion programs are not only safe but also highly efficient, with low rates of adverse events comparable to inpatient settings. This model allows hospitals to serve more patients with the same infrastructure and is a key strategy in managing the ongoing challenges of blood product inventory and staffing shortages.
Risks, Limitations, and How They Are Managed
Understanding the Universal Risks of Transfusion
It is vital to remember that a day transfusion does not change the fundamental risks of receiving blood. These include:
- Acute Hemolytic Reaction: The most serious, caused by receiving the wrong blood type. Meticulous double-checking protocols make this extremely rare (approx. 1 in 38,000 to 1 in 70,000 transfusions).
- Allergic Reaction: Ranges from mild hives to severe anaphylaxis. Pre-medication and slow initial rates help manage this.
- Febrile Non-Hemolytic Reaction: Fever and chills without blood destruction, often managed with antipyretics.
- Transfusion-Related Acute Lung Injury (TRALI): A rare but life-threatening lung complication.
- Transfusion-Associated Circulatory Overload (TACO): Fluid overload, especially risky for patients with heart or kidney failure. Patients are weighed, and transfusion rates/volumes are carefully calculated.
- Infectious Disease Transmission: The risk of HIV, hepatitis B/C, and other infections is exceedingly low (often cited as 1 in several million) due to rigorous donor screening and nucleic acid testing (NAT) of all donated blood.
Specific Considerations for the Outpatient Setting
The primary limitation of the day transfusion model is the inability to manage a serious acute reaction in an immediate inpatient setting. While all centers have emergency protocols, medications, and transfer agreements, a severe reaction would necessitate an emergency 911 call and hospital admission. This is why patient selection is so strict. There is also a small risk of a delayed reaction occurring after the patient has gone home, which is why the 24-hour contact line and clear discharge instructions are non-negotiable components of the process. Furthermore, the logistics of scheduling, staffing, and ensuring blood availability can sometimes lead to delays or cancellations on the day of the procedure.
Practical Tips for a Smooth and Successful Day Transfusion
For Patients and Caregivers
- Be Your Own Advocate: Confirm your name and date of birth with the nurse before the blood is started. It's okay to ask, "Can you please check this against my wristband?"
- Communicate Clearly: Report any sensation—itching, warmth, nausea, back pain—immediately, even if it seems minor.
- Plan Your Day: Clear your schedule. Bring distractions. Wear comfortable clothes. Arrange for a full day of rest at home afterward; even if you feel fine, your body is processing a significant volume of foreign material.
- Stay Hydrated: Drink water before, during (if possible), and after the transfusion.
- Know the Signs: Memorize the discharge instructions. Have the emergency number saved in your phone and posted visibly at home.
For Healthcare Providers Optimizing the Program
- Standardize Protocols: Have clear, evidence-based inclusion/exclusion criteria and standardized order sets.
- Invest in Education: Train all staff (nurses, transporters, lab techs) on the unique workflow and emergency response for the outpatient setting. Patient education materials must be clear and multilingual.
- Streamline Flow: Dedicate a specific area, schedule transfusion slots efficiently, and have a rapid discharge pathway for uncomplicated cases.
- Robust Follow-Up: Implement a system for a nurse-led phone call the next morning to check on patients who received a transfusion the prior day. This catches delayed reactions and builds patient trust.
- Collaborate with Blood Bank: Ensure seamless communication between the ordering physician, the infusion center, and the blood bank for timely crossmatching and unit reservation.
Frequently Asked Questions About Day Transfusions
Q: How long does a same-day transfusion actually take?
A: From check-in to discharge, expect to be at the center for 4 to 8 hours. The actual transfusion of one unit of red blood cells takes about 2-4 hours. The remaining time is for registration, IV placement, baseline checks, the initial slow-rate monitoring period, and the final observation period.
Q: Can I drive myself home?
A: Absolutely not. You will be sedated from any pre-medications and may feel fatigued. You must have a designated driver over the age of 18 who accompanies you and drives you home. They should also stay with you for the first few hours after you return.
Q: What should I do if I develop a fever or rash at home?
A: Call the emergency contact number provided by your transfusion center immediately. Do not wait. Describe your symptoms. They will advise you on whether to come to the emergency department or can sometimes manage it with phone guidance. Always mention you had a blood transfusion the day before.
Q: Are day transfusions covered by insurance?
A: Yes, in the vast majority of cases. Outpatient transfusions are billed under your medical insurance, not your pharmacy benefit. They are typically coded as a facility/outpatient hospital service. Co-pays may apply, just as they would for any other outpatient procedure. Always verify with your insurer.
Q: How many units of blood can I receive in one day?
A: This is strictly determined by your hematologist based on your weight, cardiac and renal function, and current hemoglobin level. The standard is often one unit for a stable outpatient, sometimes two units if the anemia is severe and the patient has no history of fluid overload. More than two units in a single outpatient session is uncommon due to TACO risk.
Conclusion: Embracing a Safer, More Patient-Centric Model
The day transfusion is not a compromise in care; it is an evolution in care. It represents the successful convergence of medical science, patient safety protocols, and a deep respect for the patient's life outside the hospital walls. By rigorously selecting appropriate candidates and operating within a framework of constant monitoring and clear communication, healthcare providers can offer a profoundly less disruptive alternative to traditional inpatient transfusion. For the patient with chronic anemia, this model transforms a periodic medical necessity from an isolating hospital ordeal into a manageable, scheduled appointment. It restores precious days to their lives, reduces financial and logistical strain on families, and allows the healthcare system to allocate its finite resources more effectively. If you are facing the possibility of needing regular blood transfusions, have an open conversation with your hematologist about whether a same-day outpatient transfusion program is a safe and suitable option for you. Understanding this process empowers you to be an active participant in your care plan, turning a daunting medical term into a clear, manageable pathway to feeling better.