Broken Ankle Vs Sprained Ankle: How To Tell The Difference And What To Do
Have you ever twisted your ankle and wondered, "Is this just a sprain, or did I actually break it?" That moment of sharp pain, followed by swelling and uncertainty, is something millions of people experience each year. Distinguishing between a broken ankle and a sprained ankle is crucial because the treatment pathways, recovery timelines, and potential complications differ significantly. While both are common musculoskeletal injuries, one involves damaged ligaments and the other a fractured bone—or sometimes, tragically, both. Understanding the key differences empowers you to seek the right care, avoid long-term disability, and get back on your feet as quickly and safely as possible. This comprehensive guide will walk you through everything you need to know, from the anatomy of your ankle to the definitive diagnostic tools and tailored treatment plans for each injury.
Understanding Your Ankle: A Complex Engineering Marvel
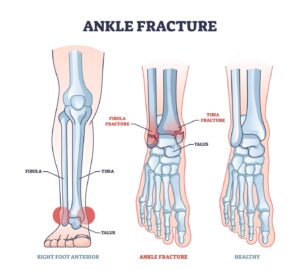
Before diving into the injuries themselves, it's essential to understand the structure you're dealing with. Your ankle is a sophisticated hinge joint where three bones meet: the tibia (shinbone), the fibula (the thinner bone alongside the tibia), and the talus (a foot bone that sits within the socket formed by the tibia and fibula). This structure is stabilized by a network of strong, fibrous ligaments that connect bone to bone, controlling movement and preventing excessive rolling or twisting. The most commonly injured ligament on the outside of the ankle is the anterior talofibular ligament (ATFL). Tendons, which connect muscle to bone, also play a vital role in ankle function. When an injury occurs, the force can impact any of these components—bones, ligaments, or tendons—leading to very different diagnoses and outcomes.
The Core Difference: Ligaments vs. Bone
At its heart, the distinction between a sprain and a break is simple but profound.
What is a Sprained Ankle?
A sprained ankle occurs when the ligaments that support the ankle are stretched beyond their normal capacity or tear partially or completely. The injury is to the soft tissue. Sprains are graded on a scale:
- Grade 1 (Mild): Microscopic tearing or stretching of ligament fibers. There is mild tenderness and swelling, but minimal instability. You can usually still bear weight.
- Grade 2 (Moderate): Partial tearing of the ligament. This results in moderate pain, swelling, and bruising. You'll experience some degree of ankle instability and difficulty bearing weight.
- Grade 3 (Severe): A complete tear or rupture of the ligament. This causes significant swelling, bruising, severe pain, and marked instability. The ankle may feel "loose" and cannot support weight.
What is a Broken Ankle?
A broken ankle, or ankle fracture, involves a break in one or more of the bones that make up the ankle joint (tibia, fibula, or talus). The fracture can be a clean break, a crack, or even a shattering of the bone. The severity is determined by the location, pattern, and whether the bones are displaced (out of their normal alignment). A fracture often occurs from a more significant force, like a fall from a height, a direct blow, or a severe twist where the bone itself gives way. Importantly, a severe sprain can cause an avulsion fracture, where a piece of bone is pulled off by the ligament or tendon that's tearing.
Comparing Causes and Mechanisms of Injury
The ways you get hurt often provide the first clue.
- Bernice Burgos Shocking Leaked Video Exposes Everything
- Edna Mode
- Leaked Porn Found In Peach Jars This Discovery Will Blow Your Mind
How Sprains Happen
Sprains are overwhelmingly the more common injury. They typically occur during inversion injuries—when the foot rolls inward, placing stress on the outer ligaments. This happens frequently in sports like basketball, soccer, and tennis during sudden changes in direction, or in everyday life from stepping off a curb incorrectly or walking on uneven ground. The force is usually rotational or lateral, targeting the soft tissue stabilizers.
How Fractures Happen
Fractures generally require a higher-energy impact. Common causes include:
- Falls: Tripping and landing directly on the ankle or foot.
- Direct Blows: Being struck by an object or during a collision.
- Severe Twists: A twist so forceful that it exceeds the bone's strength before the ligament fails.
- Overuse:Stress fractures are tiny cracks in the bone caused by repetitive force, often from suddenly increasing activity like running or jumping. These are a special category of fracture.
Symptom Showdown: Pain, Swelling, and Function
This is where the rubber meets the road for self-assessment, but remember: only a medical professional can diagnose for certain.
Symptom Checklist: Sprained Ankle
- Pain: Located primarily over the injured ligament(s), usually on the outside (lateral) of the ankle. Pain is worst with movement or pressure.
- Swelling: Develops within hours, often centered around the ankle joint. It can be significant but is usually more diffuse.
- Bruising (Ecchymosis): May appear, but often less dramatic or immediate than with a fracture. Bruising can track down into the foot and toes.
- Weight-Bearing: Often possible with a mild sprain, painful but manageable with a moderate sprain, and very difficult or impossible with a severe sprain.
- Range of Motion: Limited by pain and swelling, but the joint itself is intact.
- Deformity: None. The ankle's shape looks normal.
- Tenderness: Very specific to the ligamentous structures.
Symptom Checklist: Broken Ankle
- Pain: Intense, immediate, and directly over the broken bone. You may feel a grinding or crunching sensation (crepitus) at the time of injury.
- Swelling: Rapid and often dramatic, sometimes within minutes. Can be extensive.
- Bruising: Can be extensive and severe, sometimes appearing quickly and spreading significantly due to bleeding from the broken bone.
- Weight-Bearing: Usually impossible or causes excruciating pain. You likely cannot take a step.
- Range of Motion: Severely limited and painful in all directions.
- Deformity:This is a major red flag. You may see an obvious abnormal angle, bump, or depression in the ankle or lower leg. The bone may be visibly out of place.
- Tenderness: Directly over the fracture site. Pressing on the bone itself will cause sharp, localized pain.
- Sensation: Numbness or tingling may occur if nerves are compressed by swelling or bone fragments.
The Gold Standard: How Doctors Diagnose
Never rely on guesswork. A proper diagnosis is critical.
The Physical Examination
A doctor will perform a thorough exam, checking for:
- Deformity and Swelling Pattern.
- Point Tenderness: Pressing on specific bones (like the medial malleolus, lateral malleolus, or posterior tibia) is a key test for fracture. Tenderness over the base of the fifth metatarsal (little toe bone) suggests a common associated fracture.
- Stability Tests: Gentle maneuvers to assess ligament integrity (like the anterior drawer test for ATFL). These are avoided if a fracture is suspected.
- Neurovascular Check: Assessing pulses and sensation to ensure no damage to blood vessels or nerves.
Imaging: X-Rays and Beyond
- X-Ray: The first and most crucial tool. A standard ankle series includes views from the front, side, and an angled view. The doctor uses specific rules (like the Ottawa Ankle Rules) to determine if an X-ray is necessary. These rules state an X-ray is needed if there is bone tenderness at the posterior edge of the tibia or fibula, or at the base of the fifth metatarsal, or if you cannot bear weight immediately after the injury and take four steps.
- CT Scan: Provides a 3D cross-sectional view. It's superior for seeing complex fracture patterns, tiny bone fragments, and joint alignment. Often used for surgical planning.
- MRI: The best tool for visualizing soft tissues—ligaments, tendons, cartilage, and bone bruises. It's excellent for diagnosing high-grade sprains, occult (hidden) fractures, and assessing associated injuries. It's typically ordered if the X-ray is negative but severe pain and instability persist.
Treatment Pathways: Diverging Roads to Recovery
Treatment is where the differences become most practical and impactful.
Treating a Sprained Ankle: The RICE Principles and Beyond
The cornerstone of initial sprain treatment is the R.I.C.E. protocol:
- Rest: Avoid activities that cause pain. Use crutches if needed.
- Ice: Apply ice packs for 15-20 minutes every 2-3 hours for the first 48-72 hours to reduce swelling and pain.
- Compression: Use an elastic bandage (like ACE wrap) to provide gentle, even pressure. Don't wrap so tightly it cuts off circulation.
- Elevation: Keep the ankle raised above the level of your heart as much as possible.
Additional Treatment:
- Immobilization: A Grade 2 or 3 sprain often requires a brace, walking boot, or stirrup-style ankle support to stabilize the joint and allow ligaments to heal.
- Medication: Over-the-counter NSAIDs (like ibuprofen) can help with pain and inflammation.
- Physical Therapy:This is critical for a full recovery, especially for Grade 2 and 3 sprains. A physical therapist will guide you through exercises to restore range of motion, strengthen the muscles around the ankle (especially the peroneal muscles), and retrain proprioception (your body's sense of joint position). This is the best way to prevent chronic instability and re-injury.
- Surgery: Rarely needed for acute sprains, but may be considered for chronic instability that doesn't improve with extensive therapy, or for a ligament that has completely retracted and won't heal.
Treating a Broken Ankle: From Cast to Surgery
Treatment depends entirely on the fracture type, location, and stability.
Non-Surgical (Closed Reduction & Casting):
- If the bones are in good alignment (non-displaced), treatment is often a cast or splint for 6-8 weeks to immobilize the bone and allow it to knit together.
- Sometimes, a doctor must perform a closed reduction, a procedure to manually realign the bones before casting.
- Weight-bearing is strictly prohibited until the bone is sufficiently healed, as confirmed by follow-up X-rays.
Surgical (Open Reduction and Internal Fixation - ORIF):
- Required for displaced fractures, unstable fractures, or fractures that involve the joint surface (intra-articular fractures).
- During surgery, an orthopedic surgeon makes incisions to directly access the broken bones, realigns them (reduction), and secures them with metal hardware like plates, screws, and rods.
- The hardware is often left in place permanently unless it causes problems later.
- Post-surgery involves a period of non-weight-bearing in a splint or boot, followed by a gradual return to weight-bearing and intensive physical therapy.
The Peril of Misdiagnosis: Why Getting It Right Matters
Treating a fracture like a sprain, or vice versa, can have serious consequences.
- Undiagnosed Fracture: If you treat a fracture with just rest and a brace (sprain protocol), the broken bones will not heal properly. This leads to malunion (healing in a bad position), resulting in chronic pain, arthritis, deformity, and permanent instability. You may never regain full function.
- Unnecessary Surgery for a Sprain: While rare, subjecting someone with a severe sprain but no fracture to surgery exposes them to the risks of infection, nerve damage, and hardware complications unnecessarily.
- Long-Term Complications: Both injuries, if inadequately treated, can lead to post-traumatic arthritis in the ankle joint. A poorly aligned fracture is a direct recipe for this painful, degenerative condition years later.
Prevention: Your Best Defense
While not all injuries are preventable, you can significantly reduce your risk.
- Wear Proper Footwear: Choose shoes that fit well and are appropriate for the activity. Athletic shoes should be in good condition with adequate tread and support.
- Strengthen Your Ankles: Simple exercises like heel raises, alphabet drawing with your toes, and balance training (e.g., standing on one leg) build strength and proprioception.
- Warm-Up Before Activity: Dynamic stretches and light cardio prepare your muscles and joints.
- Be Aware of Your Environment: Watch for uneven surfaces, potholes, and debris. Use caution on stairs and in poorly lit areas.
- Consider Taping or Bracing: If you have a history of ankle sprains, using a prophylactic ankle brace or having a athletic trainer tape your ankles during sports can provide valuable external support.
- Gradual Progression: Avoid the "too much, too soon" trap. Increase the intensity and duration of workouts slowly to allow your musculoskeletal system to adapt.
When to See a Doctor Immediately: Red Flags
Do not "tough it out." Seek urgent medical attention if you experience:
- Inability to bear weight immediately after the injury or when trying to take a few steps.
- Visible deformity in the ankle or lower leg.
- Severe pain that is not manageable with over-the-counter medication.
- Numbness or tingling in the foot or toes, or a foot that looks pale or blue (signs of vascular compromise).
- A "popping" or "snapping" sound at the time of injury.
- Swelling and pain that worsen after 48-72 hours despite RICE.
Conclusion: Knowledge is Your First Step to Recovery
The battle of broken ankle vs sprained ankle is ultimately a battle for accurate diagnosis and appropriate treatment. While a sprain is a ligamentous injury treated primarily with immobilization and rehabilitation, a fracture is a bony injury that may require casting or surgery to ensure proper healing. The symptoms can overlap, but key signs like an inability to bear weight, point tenderness over bone, and especially any visible deformity point strongly toward a fracture. Your takeaway? When in doubt, get it checked out. An X-ray is a simple, non-invasive tool that provides definitive answers. Investing in a proper diagnosis from a healthcare professional—be it a primary care doctor, urgent care physician, or emergency room doctor—is the single most important step you can take to protect your long-term ankle health. Don't let uncertainty lead to a lifetime of pain; trust the experts to guide your recovery journey correctly from the very beginning.