Bell's Palsy Vs CVA: Critical Differences Every Patient Must Know
Waking up to find one side of your face suddenly drooping is a terrifying experience. Your immediate thought might be, "Is this a stroke?" But another common culprit is Bell's palsy. The urgent question "Bell's palsy vs CVA—which one is this?" isn't just medical trivia; it's a life-altering distinction. While both conditions cause facial weakness or paralysis, their origins, urgency, treatments, and long-term outlooks are worlds apart. Misidentifying one for the other can lead to catastrophic delays in care. This comprehensive guide will dismantle the confusion, arming you with the knowledge to recognize the critical signs and understand why getting the right diagnosis, as quickly as possible, is absolutely essential.
Understanding the Core Difference: Where the Problem Lives
The single most fundamental distinction between Bell's palsy and a cerebrovascular accident (CVA), commonly known as a stroke, lies in the location of the neurological damage. This isn't a minor detail; it's the root cause that dictates every other aspect of the condition.
The Peripheral Nerve Problem: Bell's Palsy
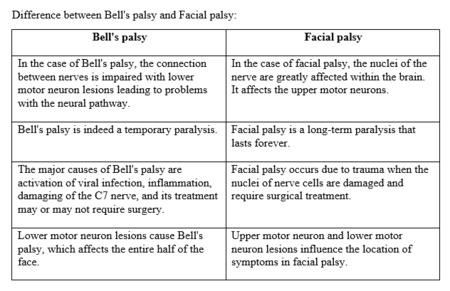
Bell's palsy is a diagnosis of exclusion that refers specifically to an acute, unilateral (one-sided) facial paralysis caused by inflammation or compression of the seventh cranial nerve, also known as the facial nerve. This nerve is peripheral, meaning it originates in the brainstem but travels a long, winding path through a narrow bony canal in the skull (the facial canal) before branching out to control all the muscles of facial expression. Think of it like a main electrical cable that gets pinched or swollen somewhere along its route outside the central brain tissue. The exact trigger is often linked to the reactivation of the herpes simplex virus (HSV-1), though other viral infections may play a role. The inflammation causes the nerve to swell and become compressed within the rigid confines of the facial canal, disrupting the signal flow from the brain to the facial muscles. This is a peripheral facial nerve palsy.
- Nude Photos Of Korean Jindo Dog Leaked The Disturbing Truth Revealed
- Chloe Parker Leaks
- Secret Sex Tapes Linked To Moistcavitymap Surrender You Wont Believe
The Central Brain Problem: Cerebrovascular Accident (CVA)
A stroke, or CVA, is a central neurological event. It occurs when blood flow to a part of the brain is interrupted, either by a blockage (ischemic stroke, ~87% of cases) or a rupture (hemorrhagic stroke, ~13%). The brain tissue deprived of oxygen and nutrients begins to die. When a stroke affects the cortical motor strip or the pathways that descend from it to control the face, it causes weakness. Crucially, the part of the brain that controls the upper face (forehead) receives bilateral input—meaning both the left and right hemispheres of the brain send signals to it. The lower face, however, receives contralateral (opposite side) input only. Therefore, a central lesion like a stroke typically spares the forehead on the affected side because the unaffected hemisphere can still send signals to lift that eyebrow. The damage is within the brain's central command center, not in the peripheral nerve itself.
The Forehead Clue: A Visual Diagnostic Key
This anatomical difference creates the most famous and clinically valuable sign for differentiating Bell's palsy vs CVA: the ability to wrinkle the forehead.
- In Bell's Palsy (Peripheral): The entire side of the face is affected, including the forehead. Patients cannot raise their eyebrow or wrinkle their forehead on the paralyzed side. The eye on that side may not close fully (lagophthalmos), which is a major concern for corneal drying and injury. The drooping is total and includes the forehead, eye, cheek, and mouth.
- In a Stroke (Central): The classic presentation is forehead sparing. The patient can often wrinkle their forehead and close their eye on the affected side because the upper facial muscles receive signals from both brain hemispheres. The weakness is predominantly in the lower half of the face—the mouth droops, and smiling is asymmetrical, but the upper face remains relatively intact. This is sometimes called a "central seven" pattern of facial weakness.
Practical Tip: The next time you suspect facial weakness, ask the person to perform two tasks: 1) Smile broadly or show their teeth, and 2) Raise both eyebrows as high as they can. Observing the symmetry (or lack thereof) in these two distinct movements provides an immediate, powerful clue.
- David Baszucki
- Why Is The Maxwell Trial A Secret Nude Photos And Porn Leaks Expose The Cover Up
- Walken Walken
Speed of Onset and Associated Symptoms: A Timeline of Clues
How the symptoms appear and what else is happening in the body offer vital diagnostic breadcrumbs.
Bell's Palsy: Rapid but Often Not Instantaneous
Bell's palsy typically reaches its maximum weakness within 48 hours, often overnight or over the course of a day. While sudden, it's not usually a "snap of the fingers" event. It is almost always isolated to the facial nerve. Key associated symptoms are local to the nerve's function:
- Pain: Often behind the ear or in the jaw on the affected side.
- Sensory Changes: Altered taste on the anterior two-thirds of the tongue, hyperacusis (sounds seem louder) due to paralysis of a tiny ear muscle.
- Eye Issues: Decreased tear production and inability to close the eye completely.
- No Limb Weakness: By definition, Bell's palsy does not cause weakness in the arms, legs, or other parts of the body.
Stroke (CVA): Sudden and Systemic
A stroke is the definition of a sudden neurological deficit. Symptoms maximize at onset. The event is a systemic brain injury, so associated symptoms are widespread and related to the specific brain region affected. Alongside potential facial weakness (with forehead sparing), look for the FAST acronym, which has been expanded to BE FAST for better detection:
- B - Balance: Sudden loss of balance or coordination.
- E - Eyes: Sudden blurred vision, double vision, or loss of vision in one or both eyes.
- F - Face: Facial droop (often with forehead sparing).
- A - Arms: Sudden weakness or numbness in one arm (or leg).
- S - Speech: Slurred speech, difficulty finding words, or incoherent speech.
- T - Time: Time to call emergency services immediately.
The presence of any of these, especially in combination with facial weakness, points strongly toward a central cause like a stroke.
Diagnostic Pathways: Different Tools for Different Problems
Confirming the diagnosis requires entirely different medical investigations, targeting the suspected site of injury.
Diagnosing Bell's Palsy
There is no single definitive test for Bell's palsy. It is a clinical diagnosis of exclusion, meaning other causes of facial paralysis must be ruled out first. The process includes:
- Detailed History & Physical Exam: To confirm the pattern of peripheral facial weakness and rule out central signs.
- Electromyography (EMG) & Nerve Conduction Studies (NCS): These tests, usually performed a few weeks after onset, assess the health of the facial nerve and muscles. They can confirm nerve damage, estimate its severity, and predict the likelihood of recovery.
- Imaging (MRI): Not routine for classic Bell's palsy, but may be ordered if the presentation is atypical (e.g., gradual onset, recurrent episodes, or presence of other neurological signs) to rule out tumors, strokes, or demyelinating diseases like MS compressing the nerve.
- Blood Tests: To screen for other potential causes like Lyme disease, HIV, or sarcoidosis if clinically suspected.
Diagnosing a Stroke (CVA)
Stroke diagnosis is urgent and protocol-driven, focused on the brain.
- Immediate Neurological Exam: Using scales like the NIH Stroke Scale (NIHSS) to quantify deficit.
- Urgent Brain Imaging:
- Non-contrast CT Scan: The first-line test in the emergency room to quickly rule out a hemorrhagic stroke (bleed).
- MRI with Diffusion-Weighted Imaging (DWI): More sensitive than CT for detecting early ischemic stroke (blockage) within minutes of onset.
- Vascular Imaging:CT Angiography (CTA) or MR Angiography (MRA) to locate a clot or vascular malformation.
- Carotid Ultrasound: To check for plaque in the neck arteries that could be the source of an embolic stroke.
- Heart Tests: EKG, echocardiogram to find cardiac sources of clots (e.g., atrial fibrillation).
The diagnostic goal for stroke is not just to confirm it happened, but to determine type and location to guide acute, time-sensitive treatments.
Treatment Protocols: Diverging Paths to Recovery
The treatment philosophies for these two conditions are opposites in urgency and approach.
Treating Bell's Palsy: Reducing Nerve Inflammation
The cornerstone of early Bell's palsy treatment is to reduce swelling of the facial nerve within its bony canal.
- Corticosteroids: A short course of prednisone (or similar), started within 72 hours of symptom onset, is the gold standard. It significantly improves the odds of full recovery by reducing inflammation and compression. The benefit is time-sensitive.
- Antiviral Agents: The role of antivirals like acyclovir or valacyclovir is debated. They are often prescribed in combination with steroids, especially for severe cases, based on the suspected HSV-1 link, though their standalone benefit is less clear.
- Eye Care: This is paramount. Since the eye may not close, patients must use lubricating eye drops during the day, ointment at night, and often an eye patch or tape the eyelid shut to prevent corneal abrasions and ulcers from drying.
- Physical Therapy: Gentle facial exercises and massage can help maintain muscle tone and prevent permanent contractures. A physical therapist specializing in facial rehabilitation can provide guidance.
- Pain Management: Over-the-counter pain relievers for associated discomfort.
Treating a Stroke: Saving Brain Tissue
Stroke treatment is a race against time. The goal is to restore blood flow or stop bleeding to save as much brain tissue as possible.
- Acute Ischemic Stroke (Clot):
- IV tPA (tissue plasminogen activator): A clot-busting drug administered intravenously within a 4.5-hour window from last known well.
- Endovascular Thrombectomy: A surgical procedure to physically remove a large clot from a major brain artery. This can be effective up to 24 hours in select patients with a large vessel occlusion.
- Acute Hemorrhagic Stroke (Bleed): Treatment focuses on controlling blood pressure, reversing any blood thinners, and often neurosurgical intervention to evacuate the hematoma or repair the aneurysm.
- Secondary Prevention & Rehabilitation: After the acute phase, the focus shifts to preventing a recurrence with medications (antiplatelets like aspirin, anticoagulants for AFib, statins, blood pressure control) and intensive rehabilitation. This includes physical, occupational, and speech therapy to regain lost functions. Recovery from stroke is often a long-term, arduous process.
Prognosis and Recovery: Vastly Different Journeys
The expected outcomes for Bell's palsy vs CVA are perhaps the most starkly different.
Bell's Palsy Prognosis: Generally Favorable
The prognosis for Bell's palsy is excellent for most people. Studies show that ~70-85% of patients show significant to complete recovery within 6 months, even without treatment. Factors associated with a poorer prognosis include:
- Complete paralysis at onset.
- Presence of pain behind the ear.
- EMG showing >90% nerve degeneration.
- Delayed treatment (beyond 72 hours for steroids).
A small percentage may have residual weakness, synkinesis (involuntary muscle movements when trying to smile), or contracture, but full recovery is the rule, not the exception.
Stroke (CVA) Prognosis: Variable and Often Challenging
Stroke prognosis is highly variable and depends on:
- Size and location of the stroke.
- Speed of treatment (time is brain).
- Patient's age and pre-stroke health.
Recovery is a marathon. While some function returns in the first few weeks (spontaneous recovery), the most significant gains happen in the first 3-6 months with dedicated rehabilitation. However, recovery can continue for years. According to the CDC, stroke is a leading cause of serious long-term disability. Outcomes range from full recovery to severe, permanent impairment affecting mobility, speech, cognition, and independence. The emotional and financial toll on patients and families is immense.
The Golden Hour: Why Speed is Non-Negotiable
This is the most critical section of any Bell's palsy vs CVA discussion. You cannot wait and see.
- If it's a stroke: Every minute of untreated blockage kills an estimated 1.9 million brain cells. Administering tPA within the 4.5-hour window can significantly reduce disability. The phrase "time is brain" is literal. Calling emergency services (911/112/999) at the first sign of a potential stroke is the single most important action a bystander can take.
- If it's Bell's palsy: While not immediately life-threatening like a stroke, starting steroids within 72 hours significantly improves the chance of a full recovery. Delaying a diagnosis also means delaying essential eye protection, risking a painful corneal ulcer.
Actionable Rule:Any new, acute facial weakness or drooping must be evaluated in an emergency department immediately. Do not assume it's "just Bell's palsy." Only a medical professional, with appropriate imaging (a CT or MRI scan), can reliably rule out a stroke. The risk of missing a stroke is far too great.
Addressing Common Questions and Misconceptions
Q: Can Bell's palsy cause a stroke?
A: No. Bell's palsy is a peripheral nerve condition. It does not increase your risk of having a stroke. However, a stroke can mimic Bell's palsy, which is why differentiation is vital.
Q: Can a stroke cause permanent Bell's palsy-like symptoms?
A: A central stroke causing facial weakness will follow the "forehead sparing" pattern. However, a very small stroke specifically in the brainstem (where the facial nerve nucleus is located) can cause a peripheral pattern of facial weakness that looks identical to Bell's palsy. This is why imaging is crucial.
Q: Is Bell's palsy contagious?
A: No. While it's associated with the herpes simplex virus (the virus that causes cold sores), Bell's palsy itself is not contagious. The virus is common and lies dormant in most people; reactivation leading to Bell's palsy is not something you can catch from another person.
Q: What is the recovery timeline for Bell's palsy?
A: Most improvement begins within 2-3 weeks, with significant recovery by 3 months. Full recovery can take up to 6-12 months. Using steroids improves the speed and completeness of recovery.
Q: Can facial exercises help both conditions?
A: Yes, but with different goals and timing. For Bell's palsy, gentle exercises started early help maintain muscle mobility and prevent stiffness. For stroke, facial rehabilitation is a critical part of long-term recovery, often guided by a speech-language pathologist or physical therapist to retrain the brain and muscles.
Conclusion: Knowledge is Your First Defense
The comparison between Bell's palsy vs CVA is more than an academic exercise; it's a roadmap for action in a moment of fear and uncertainty. The key takeaways are clear and must be remembered:
- Location is Everything:Bell's palsy = peripheral nerve problem (forehead involved). Stroke = central brain problem (forehead spared).
- Look for the Whole Picture: Stroke symptoms are systemic (FAST/BE FAST). Bell's palsy symptoms are localized to the face and its immediate functions.
- Diagnosis is Non-Negotiable: You cannot self-diagnose. A CT or MRI scan is required to rule out a stroke.
- Time is the Ultimate Factor: For stroke, call emergency services immediately. For Bell's palsy, see a doctor within 72 hours for steroids.
- Prognosis Varies Widely: Bell's palsy usually resolves. Stroke recovery is a long, hard fight with uncertain outcomes.
If you or someone you love experiences sudden facial drooping, do not hesitate. Do not "wait to see if it gets better." Seek emergency medical attention. That single, swift action could be the difference between a temporary inconvenience and a life-changing disability. Understanding these differences empowers you to act decisively, advocate for the right tests, and begin the appropriate treatment on the fastest possible timeline. In the face of facial paralysis, clarity and speed are your greatest allies.